Drug Tolerance
Reduction in response to the drug after repeated administration, characterised by the need to increase the dose in order to produce the pharmacological response of equal magnitude and duration
- Inability of the subsequent administration of the same dose, of the same drug, to be as effective as its initial dose.
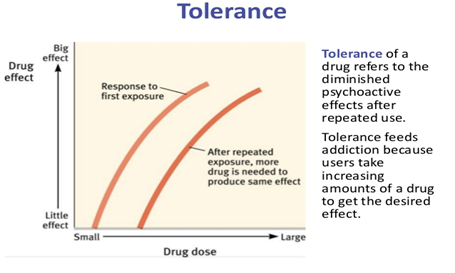
- Dose response curve shows a shift to the right as a higher dose is required to produce the same effect.
- Common phenomenon with CNS active drugs.
- Example – Tolerance develop to all effects of morphine except Miosis and Constipation
Tachyphylaxis
- Acute development of tolerance after a rapid and repeated administration of a drug at shorter intervals.
- May result due to –
- Gradual depletion of neurotransmitters from the storage vesicles
- Change in the sensitivity of the target cells
- Tachyphylaxis to nitrates
- Observed among workers in its manufacturing industry
- On Monday or Tuesday – HEADACHE due to vasodilatory effects of nitroglycerine
- Gradually disappears by Friday due to development of tolerance
- Headache reappears on Monday after weekend – “Monday disease”
- Tolerance v/s Tachyphylaxis
Tolerance
- Observed more often clinically
- Develops slowly
- Original effect of drug can still be obtained by increasing the dose
Tachyphylaxis
- Less often in clinical practice
- Develops faster
- Not possible – exhaustion of mediators or faster desensitization of target
Types of Tolerance
- Innate tolerance
- Acquired tolerance
- Pharmacokinetic tolerance
- Pharmacodynamic tolerance
- Learned tolerance
- Behavioural tolerance
- Conditioned tolerance
Innate Tolerance
- Natural or congenital
- Genetically determined lack of sensitivity to a drug
- Observed the very first time the drug is administered
- Rabbits are tolerant to large doses of atropine
- African blacks are tolerant to mydriatic action of sympathomimetics
- Chinese are tolerant to purgative action of castor oil
- Eskimos tolerate high fatty diet without any clinical consequence
Acquired Tolerance – Pharmacokinetic Tolerance
- Metabolic / drug dispositional tolerance
- Changes in the distribution or metabolism of a drug – given dose produces lower blood concentration than the initial dose
- Higher doses compensates for the losses incurred due to faster drug disposition.
- Alcohol
- It is an example of pharmacokinetic tolerance resulting due to poor absorption
- Chronic alcoholics – thickened (indurated) gastric mucosa – reduces the extent of alcohol absorption
- Barbiturates
- It is an example of pharmacokinetic tolerance due to increase in rate of metabolism
- They stimulate production of higher levels of hepatic CYPs
- Rapid removal of barbiturates from circulation
- Nitro vasodilators
- The pronounced tolerance that occurs results mainly from decreased metabolism
- Decreased metabolism – reduces the release of active metabolite Nitric Oxide
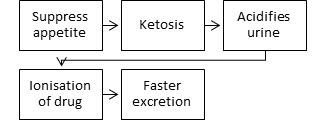
- Amphetamine
- It is an example of pharmacokinetic tolerance due to faster excretion
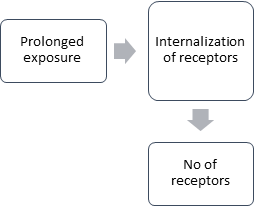
Acquired Tolerance – Pharmacodynamic Tolerance
- Adaptive changes within systems affected by the drug
- Response to a given concentration of the drug is reduced
- Translocation of receptors
- GPCR Desensitization
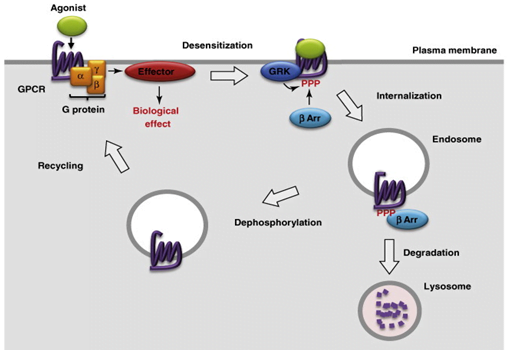
- Impairment in Receptor coupling to signal transduction pathway
- Phosphorylation of receptor interferes with its ability to activate second messenger cascades though it can still bind the agonist molecule
- Receptors directly coupled to ion channels – tolerance often rapid and pronounced
- At the Neuromuscular junction – conformational change in the receptor – tight binding of agonist molecule without opening of ion channel.
Learned Tolerance
- Reduction in effects of a drug due to compensatory mechanisms acquired by past experiences
- It includes –
- Behavioural tolerance
- Conditioned tolerance
Behavioural Tolerance
- Refers to the skills that can be developed through repeated experiences with attempting to function despite a state of mild to moderate intoxication
- Eg: Learning to walk a straight line despite the motor impairment produced by alcohol intoxication.
- Higher levels of intoxication, this tolerance is overcome.
Conditioned Tolerance
- When a drug affects homeostatic balance, there is usually a reflexive counteraction or adaptation in the direction of maintaining the status quo
- Eg: The blood pressure lowering effect of thiazide diuretics is limited because of gradual activation of renin- angiotensin system
- Drug taken in presence of environmental cues – begin to predict the effects of the drug and adaptations begins even before the drug reaches its site of action
- Prevent the full manifestation of drug’s effects. This mechanism of conditioned tolerance production follows the classical pavlonian principles of learning
- Drug received in novel or unexpected circumstances – conditioned tolerance does not occur
Reverse Tolerance
- Refers to increase in the response to a drug with repetition of same dose of the drug
- Also known as SENSITIZATION.
- It results in a shift to the left in the dose response curve.
- Repeated daily administration to rats of cocaine that produces increased motor activity, the effect increases over several days even though the dose remains constant.
Cross Tolerance
- Repeated use of a drug in a given category confers tolerance not only to that drug but also to other drugs in the same structural and mechanistic category.
- Those drugs resembling in chemical structures show cross tolerance.
- If a person is tolerant to morphine, he also shows tolerance to pethidine (synthetic derivative) and codeine.
- Complete cross tolerance is observed in cases like diazepam and flurazepam
- Incomplete cross tolerance occurs with the drugs sharing the same pharmacological properties.
- Examples include barbiturates and general anaesthetics – site of action is CNS, incomplete cross tolerance may be observed although they are not resembling chemically, but having same pharmacological properties.
- Sometimes cross tolerance occurs between two drugs that do not share mechanisms of action or classification
- Eg: Alcohol exhibit cross tolerance with nicotine in animal models – possible in humans
- Amphetamine exhibit cross tolerance with caffeine
Clinical implications of tolerance
- Regular use of inhaled β-agonist leads to tolerance to its bronchoprotective effect.
- Eg- Salbutamol , salmeterol
- Increase the dose of salbutamol
- Combining salbutamol with ipratropium bromide
- Tachyphylaxis to nitrates
- Generation of tachyphylaxis can be suppressed or even avoided by supplementation of appropriate antioxidants (SOD, vitamin C)
- Even fully developed tolerance (during non-intermittent GTN-administration) could be reversed by starting an appropriate antioxidant supplementation.
- Tolerance leads to treatment failure and progression of disease
- Prompt early recognition and appropriate alternative drug treatment helps patients
- Abused drugs – can lead to fatal overdoses due to tolerance