Erectile dysfunction and Ejaculatory Dysfunction
- Three of the most common male sexual dysfunctions are decreased libido, erectile dysfunction (ED), and ejaculatory dysfunction (including premature ejaculation [PE] in men ages 18 to 59 years).
- One or more conditions can coexist in an individual.
- The inability to achieve and/or maintain an erection sufficient for satisfactory sexual intercourse is a distressing and common symptom, affecting up to one-third of adult men.
- ED is common in men with systemic disorders such as hypertension, ischemic heart disease, and diabetes mellitus, and its prevalence increases with age
General principles
- Therapy of men with sexual dysfunction is aimed at improving libido and addressing the two vital sexual functions: the capacity to acquire and sustain penile erections and treating premature ejaculation (PE).
management approach —
●Identifying the underlying etiology, including drugs such as antidepressants or antihypertensive agents that may be causing or contributing to the erectile dysfunction (ED).
| Vascular | Cardiovascular disease, hypertension, diabetes mellitus, hyperlipidemia, smoking, major surgery (radical prostatectomy) or radiotherapy (pelvis or retroperitoneum) |
| Neurologic | Spinal cord and brain injuries, Parkinson disease, Alzheimer disease, multiple sclerosis, stroke, major surgery (radical prostatectomy) or radiotherapy of the prostate |
| Local penile factors | Peyronie’s disease, cavernous fibrosis, penile fracture |
| Hormonal | Hypogonadism, hyperprolactinemia, hyper- and hypothyroidism, hyper- and hypocortisolism |
| Drug induced | Antihypertensives, antidepressants, antipsychotics, antiandrogens, recreational drugs, alcohol |
| Psychogenic | Performance-related anxiety, traumatic past experiences, relationship problems, anxiety, depression, stress |
●Identifying and treating cardiovascular risk factors such as smoking, obesity, hypertension, and dyslipidemia
Lifestyle changes —
- Both lifestyle modification (weight loss, physical activity) and medical management of cardiovascular risk factors are effective for improving sexual function in some men with ED
- There is evidence that smoking increases the risk of ED and that stopping smoking can be beneficial
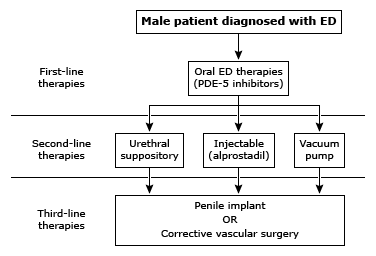
Phosphodiesterase-5 inhibitors —
- first-line therapy of ED,
- because of their efficacy, ease of use, and favorable side-effect profile.
- Sildenafil, vardenafil, tadalafil, and the newest option, avanafil, appear to be equally effective, but tadalafil has a longer duration of action and avanafil has a more rapid onset
- The rationale for the use of PDE5 inhibitors is based upon the role of nitric oxide-induced vasodilation, which is mediated by cyclic guanosine monophosphate (GMP) in initiating and maintaining an erection; detumescence is associated with catabolism of cyclic GMP by the PDE5 enzyme.
- PDE5 inhibitors act by increasing intracavernosal cyclic GMP levels by competitively inhibiting the PDE5 enzyme and, as a result, increase both the number and duration of erections in men with ED
- Sexual stimuli needed for initial nitric oxide release
- PDE inhibitors are contraindicated in men taking nitrates and should be used cautiously in men receiving an alpha-adrenergic blocker.
- An important factor in the success of PDE5 inhibitor therapy is instruction and counseling on proper use, including onset of action of the drug and taking medications on an empty stomach
- Repeat challenge with proper instruction and counseling of patients labeled as PDE5 inhibitor failures has been demonstrated to salvage approximately 25 to 30 percent of patients who were apparent initial non-responders to PDE5 inhibitor therapy
Sildenafil —
- For maximum effectiveness, sildenafil should be taken orally on an empty stomach approximately one hour before a planned sexual encounter.
- The initial dose should be 50 mg, and it should be reduced to 25 mg if side effects occur.
- If, on the other hand, it is well tolerated but the erectile response is not fully satisfactory, the dose can be increased to 100 mg.
- The duration of action is approximately four hours
Vardenafil —
- Vardenafil shares a similar structure, onset, and duration of action and side-effect profile with sildenafil
- Its duration of action, like sildenafil, is approximately four hours
- available as a 10 and 20 mg dose,
- new formulation àorally disintegrating tablet à potentially more rapid onset
- High-fat, but not moderate-fat, meals may lower vardenafil’s peak serum concentration by approximately 18 percent and delay its absorption by one hour.
Tadalafil —
- Tadalafil has a different chemical structure than sildenafil and vardenafil
- as effective as sildenafil and vardenafil, but it has a longer duration of action
- recommended starting dose for as-needed use is 10 mg, decreasing to 5 mg or increasing to 20 mg if necessary
Avanafil —
- newer PDE5 inhibitor that has been approved in the United States and Europe.
- has enhanced PDE5 selectivity compared with the other PDE5 inhibitors,
- more rapid onset of action
- starting dose of 50 mg, increasing to 100 and 200 mg as needed.
- The 50 mg dose should be taken 30 minutes before sexual activity, while the 100 to 200 mg doses can be taken just 15 minutes in advance
- Avanafil is the only PDE5 inhibitor approved for 15-minute onset of action.
Choice of drug —
All four PDE5 inhibitors (avanafil, sildenafil, vardenafil, and tadalafil) work to sustain levels of cyclic GMP within the penile corpora cavernosa to allow men with ED to achieve erections in response to appropriate sexual stimuli.
choice of PDE5 inhibitor be based upon on the patient’s preferences, including cost, ease of use, desired duration of action, and adverse effects
Sildenafil has the longest safety record of the four drugs.
Sildenafil and vardenafil must be taken on an empty stomach (high-fat meals and alcohol delay absorption).
Food does not interfere with the absorption of tadalafil, avanafil, or ODT vardenafil
Adverse effects and precautions
Cardiovascular —
Sildenafil à vasodilator that can lower the blood pressure, and it can interact with nitrates.
PDE5 inhibitors are contraindicated in patients taking nitrates of any form
Nitrate treatment should be delayed if a man who has taken a PDE5 inhibitor develops chest pain. The delay should be 24 hours if he has taken sildenafil or vardenafil and 48 hours if tadalafil; the delay should be longer for each if he has renal or hepatic dysfunction.
Alpha-adrenergic antagonists, which are commonly used for the treatment of BPH, may cause symptomatic hypotension when taken in combination with PDE5 inhibitors these drugs include terazosin, doxazosin, tamsulosin, alfuzosin, and silodosin . Tamsulosin and silodosin are better choices (ie, less or no hypotension) than doxazosin or terazosin
Myocardial infarction and sudden death have been described with and after intercourse, both in men who have and have not taken a PDE5 inhibitor. Thus, the relation to the drug is uncertain.
Higher doses of PDE5 inhibitors are used for patients with pulmonary hypertension as monotherapy or in combination with other agents, such as guanylate cyclase stimulants (eg, riociguat). However, the US Food and Drug Administration (FDA) has issued a warning against this combination because of an excess risk of hypotension.
Common side effects —
flushing, headaches, and dyspepsia, Nasal congestion
Visual effects — Sildenafil occasionally causes “blue vision” in men. The PDE5 inhibitor in sildenafil cross reacts with the PDE6 inhibitor, which is present in the retina and plays a role in color vision.
“Blue vision” has been reported in approximately 3 percent of sildenafil-treated men, lasts two to three hours, and disappears spontaneously.
Blue vision has not been reported with vardenafil, tadalafil, or avanafil
Rare cases à nonarteritic anterior ischemic optic neuropathy (NAION) were reported in men taking sildenafiland tadalafil
Hearing loss — Sildenafil, vardenafil, and tadalafil use have been associated with rare reports of sudden hearing loss Although no causal relationship has been demonstrated, the FDA requires that labeling of all PDE5 inhibitors include this potential risk
The hearing loss is usually unilateral, occurs with the first 24 hours of drug administration, and is temporary in approximately one-third of patients
Role of testosterone —
Testosterone is an important regulator of sexual desire and sexual function in men. ED and low testosterone levels often coexist in middle-aged and older men.
Measurement of serum testosterone is recommended by for men with ED and testosterone replacement has been shown to improve libido, sexual activity, and erectile function in hypogonadal men
As a result, combination therapy with a PDE5 inhibitor and testosterone has become increasingly common
Second-line therapies —
If PDE5 inhibitors are ineffective, we recommend vacuum erection devices, penile injections with vasodilating agents, or intraurethral alprostadil as second-line therapy.
We often suggest trying a vacuum device first because it is noninvasive and less expensive than the other options.
Vacuum-assisted erection devices —
A vacuum-constrictor device causes an erection by creating a partial vacuum around the penis, which draws blood into the corpora cavernosa.
The vacuum erection device may be used with oral PDE5 inhibitors to augment an insufficiently rigid erection post-ingestion of the PDE5 inhibitor
Vacuum erection devices should only be applied for a maximum for 30 minutes.
Vacuum devices successfully create erections in as many as 60 to 70 percent of patients.
Penile self-injection —
- Intracavernosal injection therapy with alprostadil (prostaglandin E1) and papaverine have been used for purposes of inducing erection
- In the United States, prostaglandin E1 is the only FDA-approved drug for penile self-injection.
- vasodilatory properties à injected into the corpora cavernosa à inhibit or override sympathetic vasoconstriction and act as direct smooth muscle vasodilators. à The relaxation of the smooth muscle trabeculae within the penile erectile bodies leads to an increase in blood flow to the penis.
- Some clinicians prefer compounded mixtures of phentolamine and papaverine (Bimix); prostaglandin E1 is sometimes added as a third component (Trimix).
- It should be noted that compounded penile injections are considered off-label use.
- All penile injections, à increase the risk for penile plaque development, and patients should be counseled about this potential risk.
Priapism —
- prolonged erection lasting more than four to six hours
- medical emergency
- Prolonged erections occur in 6 percent of men who use intrapenile alprostadil and approximately 11 percent of those who use intrapenile papaverine
Intraurethral alprostadil —
less invasive alternative to intrapenile injection
After insertion of the alprostadil into the urethra à the penis is massaged for up to one minute to ensure equal distribution in the corpora cavernosa.
less effective than penile injections; it also causes penile pain and bleeding in many men.
Surgical options
Surgical management of ED should be reserved for men who cannot use, or who have not responded to, first- and second-line therapies
- Penile prostheses
- Penile revascularization
Therapies for psychogenic ED
Psychotherapy –
ED is a common symptom of depression, and erectile function may be restored as psychotherapy or antidepressant drugs alleviate the depression.
However, some of the most effective antidepressant drugs of the SSRI class (eg, fluoxetine, sertraline, paroxetine) decrease both libido and erectile function
However, SSRIs can cause delayed ejaculation, an effect that is beneficial for men with premature ejaculation (PE).
Psychological counseling, including the use of sensate focus exercises by both partners, can be helpful for men with performance anxiety.
●Yohimbine –
blocks presynaptic alpha-2-adrenergic receptors, resulting in increased cholinergic and decreased adrenergic tone, has also been used for the management of psychogenic ED.
We suggest not using yohimbine, given the limited data for efficacy and the availability of effective alternatives (PDE5 inhibitors).
EJACULATORY DISORDERS
Premature ejaculation
Management depends upon the etiology, but the mainstays of therapy [132] include
- selective serotonin reuptake inhibitors (SSRIs)
- Available agents and dosages include paroxetine (10 to 40 mg/day), sertraline (50 to 200 mg/day), fluoxetine (20 to 40 mg/day), citalopram (20 to 40 mg/day), and escitalopram (10 to 20 mg/day)
- topical anesthetics
- and psychotherapy when psychogenic and/or relationship factors are present
- Phosphodiesterase (PDE) inhibitors may also be effective for the treatment of PE, but mainly in men with PE and coexisting ED