2 classes of antithrombotic drugs: antiplatelet and anticoagulant.
Antiplatelet agents: prevent platelet aggregation & clumping à prevent clots from forming
Anticoagulants: slow down clotting à attenuate fibrin formation à prevent clots from growing
Limitations of present drugs:
Narrow therapeutic index.
Drug interactions.
Problem of genetic variations l/t resistance.
Many require monitoring and many are parenterally administered.
RA in anticoagulants
Oral heparin: SNAC heparin: A phase 3 trial was conducted in patients undergoing hip replacement surgery and the active comparator was enoxiparin. The trial failed since there was increased incidence of DVT and PE and high discontinuation rate d/t nausea.
Semuloparin:
Ultra low molecular wt heparin, given by s.c. route.
T1/2 is 20 hrs and hence single dose dialy can be given.
It is being evaluated in several clinical trials like SAVE-HIP, SAVE-KNEE, SAVE-ABDO in which it is used in hip replacement surgery, knee replacement sx and abdominal and pelvic Sx resp. It is being compared to enoxiparin.
Tecarfarin: Oral Vitamin K antagonist. Metabolized by esterases and not by CYP (hence has no drug interactions and genetic variations which is the problem with warfarin). It is being evaluated in a phase 2 trial in patients of AF.
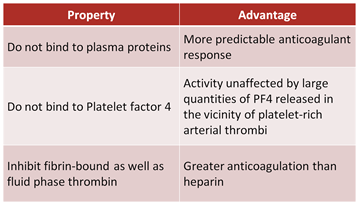
Direct thrombin inhibitors
Dabigatran etexilate: oral. Prodrug. Releases dabigatran after breakdown by esterases. Substrate of P-gp hence shows increased levels when co-administered with quinidine and amiodarone. Approved in 2010 for prevention of stroke in AF.
Flovagatran: Phase 2 in CRF patient
Pegmusirudin: PEG attached to recombinant hirudin. Being evaluated in CRF patients undergoing hemodialysis.
Factor Xa inhibitors
Idrabiotaparinux: Hypermethylated version of fondaparinux. F is given Od. Idrabiotaparinux has a long half life and hence is given once weekly. Is being evaluated in phase 3 trial in patients of symptomatic PE in comparison to warfarin. Endpoint is: Recurrent venous thromboembolism at 99 days after randomization.
Rivaroxaban: Oral Xa inhibitor. BA of 80%. Approved for 2 indications: Prophylaxis of stroke in AF. Prophylaxis of PE in patients undergoing hip and knee replacement Sx.
Apixaban: Oral. Undertrial for 2 indications: Prophylaxis of stroke in AF. Prophylaxis of PE in patients undergoing knee replacement Sx.
Edoxaban: Oral. Phase 3 trial for Prophylaxis of stroke in AF.
Otamixiban: I.v. Being evaluated for NSTEMI.
Drotrecogin alfa: It is an activated protein C (APC). Was approved for t/t of sepsis in patients of organ dysfunction. But was withdrawn since a chochrane meta-analysis did not show any survival benefir.
Presently it is undergoing Phase 2 trial in patients of acute pulmonary embolism. It is being compared as follows: : Drotrecogin plus Enoxaparin(4 dose escalating groups) compared with Enoxaparin alone.
Antiplatelet agents: (From notes)
Clopidogrel resistance: the persistent activity of clopidogrel target (i.e. P2Y12 receptors of the platelet) despite an adequate antiplatelet regime. Might be d/t CYP2C19*2 allele or co-admin with omeprazole. Genetic testing is recommended in: Those undergoing multi vessel PCI procedure, stent thrombosis, co-morbidities like DM or CRF.
Thrombin receptor antagonists: Thrombin acts on PAR receptors on the platelet membrane and activates it. This increases platelet aggregation. Atopaxar and vorapaxar are selective PAR-1 receptor antagonists. Rationale is: there is not effect on ADP induced or collagen induced platelet aggregation ie.e normal aggregation is not inhibited and hence no affection of BT, PT and aPTT. No affect of PAR4 R function.
Vorapaxar trial was stopped d/t increased ICH in stroke patients. However, another trial is going on with patients with a history of stroke being excluded.
Atopaxar: Phase 2 trial is done which has shown no increase in bleeding rate.
ADP antagonist:
Cangrelor: iv. T1/2 of 3-6 minutes. Full recovery of platelet function in 60 mins. However both trials are halted.
Ticagrelor: Reversible inhibition of P2Y12 receptors. Approved in July 2011 for reducing CV death & MI in patients of acute coronary syndrome.
Elinogrel: reversible P2Y12 antagonist. Currently ongoing in patients undergoing elective PCI.
Sarpogralte: platelet 5HT2A receptor antagonist: Compared to aspirin for recurrence of cerebral infarction. Non-inferior to asprin.
Terutroban: T for T: Terutroban is a thromboxane receptor antagonist. Blocks thromboxane-induced platelet aggregation and vasoconstriction.