Cannabinoids
- Cannabis sativa, the hemp plant: Tetrahydrocannabinol (THC) is the main active principle of cannabis
- The most abundant cannabinoids are THC,
- its precursor cannabidiol, and cannabinol, a breakdown product formed spontaneously from THC
- Cannabidiol and cannabinol lack the psychoactive properties of THC but can exhibit anticonvulsant activity.
Three general types of cannabinoids:
- Endogenous cannabinoids
- Herbal cannabinoids à present in the Cannabis plant
- Synthetic cannabinoids
Cannabinoid receptors
- Two types – CB1 receptors and CB2 receptors
Location
CB1 not homogeneously distributed, being concentrated in the
- hippocampus (relevant to effects of cannabinoids on memory),
- cerebellum (relevant to loss of coordination),
- the hypothalamus (important in control of appetite and body temperature),
- substantia nigra, mesolimbic dopamine pathways à implicated in psychological ‘reward’
- the relative paucity of CB1 receptors in the brain stem, consistent with the lack of serious depression of respiratory or cardiovascular function by cannabinoids.
CB2 receptor
- located mainly in lymphoid tissue (spleen, tonsils, and thymus as well as circulating lymphocytes, monocytes, and tissue mast cells).
- also present on microglia – immune cells in the CNS which when activated contribute to chronic pain
- typical members of the family of G protein-coupled receptors
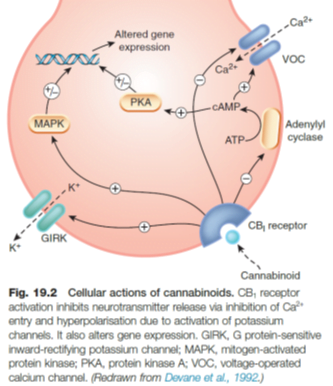
- CB1 receptors are linked via Gi/o to inhibition of adenylyl cyclase and of voltage-operated calcium channels, and to activation of G protein-sensitive inwardly rectifying potassium (GIRK) channels, causing membrane hyperpolarization.
- CB1 receptors are located in the plasma membrane of nerve endings and inhibit transmitter release from presynaptic terminals, which is caused by depolarization and Ca2+ entry.
PHARMACOLOGICAL EFFECTS
- Actions on the central nervous system include both depressant and psychotomimetic effects
- A sensation of relaxation and well-being, similar to the effect of ethanol but without the accompanying recklessness and aggression.
- impairment of short-term memory and simple learning tasks
- impairment of motor coordination (e.g. driving performance)
- catalepsy – the adoption of fixed unnatural postures
- hypothermia
- analgesia
- antiemetic action
- increased appetite
- reduction of intraocular pressure
- bronchodilatation.
TOLERANCE AND DEPENDENCE
- Tolerance to cannabis and physical dependence occur only to a minor degree and mainly in heavy users.
- Cannabinoids are less liable than opiates, nicotine or alcohol to cause dependence but may have long-term psychological effects.
ENDOCANNABINOIDS
- Anandamide CB1 > CB2
- Virodhamine CB2 > CB1
- They are eicosanoid mediators
- The main enzyme that inactivates anandamide is fatty acid amide hydrolase (FAAH).
- FAAH ‘knockout’ mice have an increased brain content of anandamide and an increased pain threshold; selective inhibitors of FAAH have analgesic and anxiolytic properties, implicating endocannabinoids in nociception and anxiety
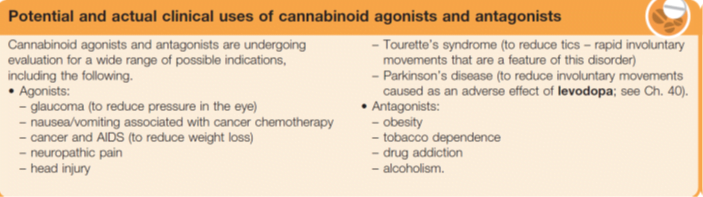
SYNTHETIC CANNABINOIDS and their clinical application
- Cannabinoid receptor agonists were developed in the 1970s in the hope that they would prove useful nonopioid/ non-NSAID analgesics respectively, for limitations of opioids and NSAIDs), but adverse effects, particularly sedation and memory impairment, were problematic
- Nabilone: sometimes used clinically for nausea and vomiting caused by cytotoxic chemotherapy if this is unresponsive to conventional antiemetics
- The first selective CB1 receptor antagonist, rimonabant à was licensed in Europe for treating obesity,
- was withdrawn because it caused psychiatric problems including depression.
- both the UK and the USA cannabinoids have been used as antiemetics
- encourage weight gain in patients with chronic diseases such as HIV-AIDS and malignancy.
- Cannabis extract (Sativex) is used to treat spasticity in patients with multiple sclerosis
Cannabidiol
- Approved June 2018
- specifically indicated for the treatment of seizures associated with Lennox Gastaut syndrome (LGS) or Dravet syndrome (DS) in patients 2 years of age and older.
- the anticonvulsant effect in humans is unknown.
- Cannabidiol DOES NOT appear to exert its anticonvulsant effects through interaction with cannabinoid receptors.