PHARMACOTHERAPY OF ACNE
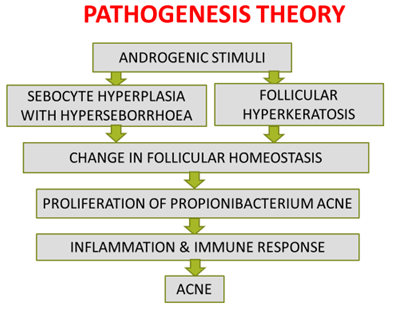
- Acne is a chronic inflammatory disorder affecting the pilosebaceous unit leading to non-inflammatory and inflammatory lesions.
- Affects nearly 10% of the global population
- 85% boys % & 83% girls affected in adolescent & young adult life
- Occurs around puberty
- Severity peak age 16 to 17 years in females & 17 to 19 years in males
- Commonly involved sites à face, chest, upper back, upper arms.
| Preadolescent | 7 year to 12 years or before menarche in girls |
| Adolescent | 12 year to 19 years or after menarche in girls |
| Persistent | Onset in adolescence and continuing after 25 years |
| Late-onset | Onset after 25 years |
Types –
- Non-InflammatoryComedones
- Open Closed
- Inflammatory
- Papule, pustule, nodule, and cyst
Treatment
Topical Antibiotics
- Slower acting, less effective than oral antibiotics.
- Clindamycin and erythromycin of 1% to 4% with or without the addition of zinc.
- Dapsone 5% gel (1995)
- No monotherapy
- Discontinuation once improvement
- No improvement within 6 to 8 weeks, discontinuation and alternate therapy
- Erythema, itching, dryness, and burning.
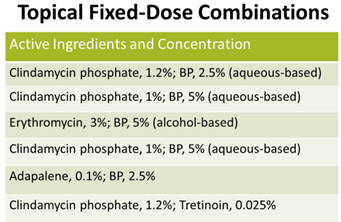
BENZOYL PEROXIDE
- Highly reactive oxygen species
- Cytotoxicity of PMNLs.
- Effective comedolytic and keratolytic agent
- Highly lipophilic
- 2.5%, 5% and 10% concentrations as gels, aquagels, creams and lotions.
- Prevents the development of resistance
- Oily skin advised to use gels, washes or solutions having a drying effect
- Dry or sensitive skin àprefer a cream formulation.
Systemic Antibiotics
- Tetracycline or oxytetracycline 250–500 mg BD for 4–6 months
- Doxycycline is at 50–100 mg BD or a single daily dose of 100 mg for 4–6 months
- Minocycline 50–100 mg BD
- Erythromycin 500 mg BD for 4–6 months.
Oral Isotretinoin
- Start at a dosage of 0.5 mg⁄ kg daily.
- severe papulopustular acne ⁄ moderate nodular acne
- Not recommended for patients under 12 years of age.
- Monitor liver enzymes and lipids, before treatment, 1 month after starting, every 3 months thereafter.
- Duration of therapy should be at least 6 months
- Avoid laser treatment, peeling and wax epilation for at least 6 months after stopping therapy.
For Acne in PCOS
FDA approved
- Norgestimate 180/215/250 mcg + 35mcg Ethinyl estradiol
- Norethindrone acetate 1 mg + EE 20/30/ 35mcg 7 day
Peeling agents
- Rationale: Controlled chemical-induced injury to the skin promoting regeneration and remodeling
- Comedonal, papulopustular:
- 20-30% Salicylic acid,
- 70% Glycolic acid
- 40-60% Pyruvic acid
- 20-25% Mandelic acid
- Jessner’s solution
- 10% Trichloroacetic acid
PHOTODYNAMIC THERAPY
- Photosensitizer, 5-aminolevulinic acid or methyl aminolevulinate
- Accumulate selectively à sebaceous glands
- Decreases size and function of sebaceous glands
- Anti-inflammatory effects, and down-regulates immune response
- Pain with illumination, erythema, and edema.
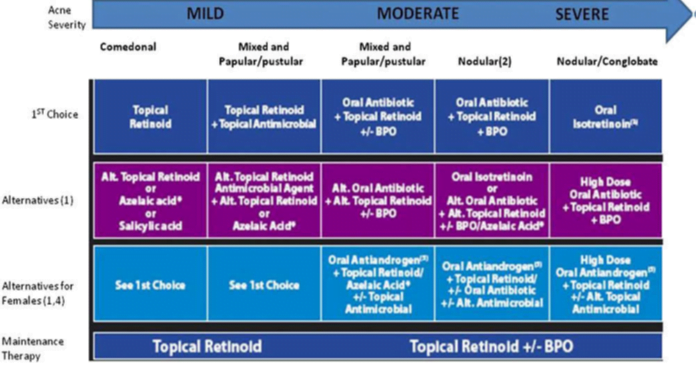
Guidelines
Strategies for limiting antibiotic resistance
- Combine a topical retinoid plus an antimicrobial
- Use of antibiotics to short periods
- Co-prescribe a BPO-containing product or use as the washout
- Oral and topical antibiotics should not be used as monotherapy
- Concurrent use of oral and topical antibiotics should be avoided
- Use topical retinoids for maintenance therapy
- Avoid the use of antibiotics for maintenance therapy