Osteoporosis
- Osteoporosis is a disease that is characterized by low bone mass, deterioration of bone tissue, and disruption of bone microarchitecture.
- The WHO operationally defines osteoporosis as a bone density that falls 2.5 standard deviations (SD) below the mean for young healthy adults of the same sex—also referred to as a T-score of –2.5.
Bisphosphonates
- inhibitory effect on osteoclast mediated bone resorption.
- accelerate apoptosis of osteoclasts and also suppress differentiation of osteoclast precursors to mature osteoclasts (by inhibiting IL-6).
- results due to reduction in cholesterol synthesis via inhibition of farnesyl pyrophosphate synthase by bisphosphonates.
- first generation à (least potent) like medronate, clodronate and etidronate
- second generation drugs like alendronate, ibadronate and pamidronate and
- third generation compounds like risedronate and zoledronate (most potent).
used for the treatment of
- post-menopausal and steroid induced osteoporosis,
- Paget’s disease and
- hypercalcemia of malignancy (pamidronate and zoledronate by i.v route are preferred).
- Bisphosphonates can also be used in malignancies.
- Zoledronate has been used successfully as an adjunct in treating philadelphia-chromosome positive CML.
- Distinctive toxicity à esophageal irritation that can lead to ulceration as well. To prevent this complication, patients taking bisphosphonates are advised to take nothing by mouth except water and not to lie down at least for half an hour. This minimizes the chances of the drug touching the esophagus.
- Zoledronate has been associated with renal toxicity and first generation bisphosphonates can result in osteomalacia.
- Recently, osteonecrosis of jaw has been noted with use of bisphosphonates particularly zolendronate.
- Patients receiving bisphosphonates must receive regular dental care and try to avoid dental extraction.
- Long-term use of bisphosphonates increases the risk of atypical ‘chalkstick’ fracture of femur (subtrochantric or shaft). Risk increases with concurrent high dose steroid therapy.
- Long-term use of bisphosphonates increase the risk of esophageal cancer.
- Bisphosphonates can result in hypocalcemia as well as hypercalcemia.
- Half-life of alendronate in bone is 10 years.
- Main contraindications of bisphosphonates are renal dysfunction, esophageal motility disorders and peptic ulcer.
- Zoledronate infusion of 5mg once yearly has been approved for treatment of osteoporosis.
Selective Estrogen Receptor Modulators
- Estrogens inhibit bone resorption directly by inhibiting osteoclasts and indirectly by modulating paracrine factors.
- increases anti-resorptive [IGF-1 and TGF-β] and suppresses pro-resorptive [IL-1, IL-6, TNF-α and osteocalcin] factor synthesis by osteoblasts.
- Estrogen increases bone formation and its deficiency in the old age may result in postmenopausal osteoporosis.
- Use of hormone replacement therapy for this condition predisposes the patients to the adverse effects of estrogens on breast and endometrium (increased incidence of breast and endometrial carcinoma).
- Raloxifene is a selective estrogen receptor modulator with estrogen agonistic action on bone and antagonistic action on breast and endometrium.
- It is therefore the preferred drug for the treatment and prevention of post-menopausal osteoporosis.
- Major adverse effect of this agent is increased risk of thromboembolism.
- Bazedoxifene is another SERM that has been approved recently for prevention of post menopausal osteoporosis and to treat vasomotor symptoms of menopause.
- Estrogen replacement therapy (ERT) is used for the treatment of postmenopausal osteoporosis when:
- a significant risk of osteoporosis.
- non-estrogen medications not considered appropriate.
- Estrogen not to be used for prevention of osteoporosis.
Teriparatide and Abaloparatide
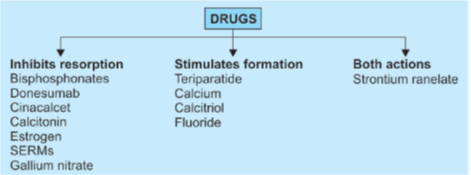
- Teriparatide, abaloparatide and strontium ranelate can stimulate osteoblast whereas most other agents used for osteoporosis act by inhibiting osteoclast
- recombinant PTH1-34.
- PTH in low and pulsatile dose stimulates bone formation whereas in excess it causes resorption of bones.
- Teriparatide is available for the treatment of osteoporosis by intermittent s.c. administration.
- stimulates the production of new collagenous bone matrix that must be mineralized. Therefore, patients receiving teriparatide must have sufficient intake of vitamin D and calcium.
- When administered to patients with osteoporosis in doses of 20 mcg/d subcutaneously for 2 years, Teriparatide dramatically improves bone density in most bones except the distal radius.
- The recommended dose should not be exceeded, since Teriparatide has caused osteosarcoma in rats when administered in very high doses. Due to potential risk of osteosarcoma, teriparatide should be avoided in:
- Paget’s disease of bone
- Prior radiotherapy to bone
- Past history of osteo or chondrosarcoma
- Unexplained increase in alkaline phosphatase
- Teriparatide should be used with caution in patients if they also taking corticosteroids and thiazide diuretics along with oral calcium supplementation because hypercalcemia may develop.
- Following a course of Teriparatide, a course of bisphosphonates should be considered in order to retain the improved bone density.
- Other adverse effects have included exacerbation of nephrolithiasis and elevation of serum uric acid levels.
- Teriparatide may be used for healing of chalkstick fractures associated with bisphosphonate therapy.
Denosumab
- Osteoclasts express a receptor called receptor for activated nuclear factor k B (RANK) on its surface.
- When this receptor is stimulated by RANK ligand, bone resorption results due to activation of osteoclasts.
- Denosumab is a monoclonal antibody against this ligand and is useful for the treatment of osteoporosis. (prevents binding of RANK-L to osteoclasts).
- It can also prevent osteoporosis. It can decrease serum calcium therefore avoided in patients with hypocalcemia.
- It has recently been approved for unresectable giant cell tumor of bone.
Cinacalcet
- Calcium sensing receptors (CaSR) are present on parathyroid gland that regulates the secretion of PTH.
- Ca2+ activates these receptors and decreases PTH secretion.
- Hypocalcemia will have opposite effect i.e. increased PTH secretion.
- Cinacalcet acts as a calcimimetic drug by directly activating calcium sensing receptors on parathyroid gland.
- It has been approved for the treatment of secondary hyperparathyroidism (due to chronic renal disease) and for patients with hypercalcemia associated with parathyroid carcinoma.
Etelcalcetide
new CaSR agonist à indicated for i.v. treatment of sec. hyperparathyroidism with CKD on hemodialysis.
Strontium ranelate
- novel mechanism of action as it inhibits bone resorption as well as stimulates bone formation.
- Strontium is incorporated into hydroxyapatite, replacing calcium.
- Small increased risk of venous thrombosis, seizures and abnormal cognition have been seen and require further studies.
Other Drugs
Calcium and calcitriol (vitamin D)
- can be used in the prophylaxis and treatment of osteoporosis.
- Calcium can be life-saving in extreme hyperkalemia (> 7 mEg/L).
- It can reverse some of the cardiotoxic effects of K+.
- Calcium is also approved for i.v. treatment of black widow spider envenomation and magnesium toxicity.
Gallium nitrate
- inhibits bone resorption and is useful in the management of Paget’s disease and hypercalcemia of malignancy
- nephrotoxicity limits its use for this indication.
Fluorides are used to prevent dental caries but their usefulness in osteoporosis is uncertain.
Thiazides
- inhibit the renal excretion of Ca2+ and thus can be used for the treatment of osteoporosis (apart from their use in recurrent calcium stones due to hypercalciuria).
Calcitonin
- inhibits resorption of bone and thus can be used for the treatment of osteoporosis.
- can be administered by nasal route for this indication.
- Calcitonin possess analgesic effects on bone pain from fractures.